3871 Maryland Medicaid PDF Template
When navigating the complex realm of medical assistance, understanding the right forms and procedures is crucial for securing the necessary support and services. Embedded within the labyrinth of health care bureaucracy in Maryland, the 3871 Maryland Medicaid form emerges as an essential document. Crafted to meticulously evaluate an individual’s medical eligibility for various levels of care, this form serves as a linchpin in accessing the broad spectrum of services offered through the Maryland Medical Assistance Program. With sections demanding detailed information regarding the applicant’s medical and rehabilitation needs, including a comprehensive physician’s plan of care, this form acts as a gateway for individuals seeking assistance with rehab hospitals, nursing facilities, medical day care, and other specialized services. It delves into patient demographics, health conditions requiring immediate attention, ongoing treatments and medication, along with an assessment of the patient's rehabilitation potential and discharge plans. Moreover, it evaluates functional and cognitive status, addressing the need for assistive devices or adaptive equipment, thereby painting a full picture of the patient's current health status and care requirements. For both patients and health professionals, understanding the nuances of the 3871 form is a step toward ensuring the delivery of appropriate care and support within Maryland’s healthcare framework.
3871 Maryland Medicaid Sample
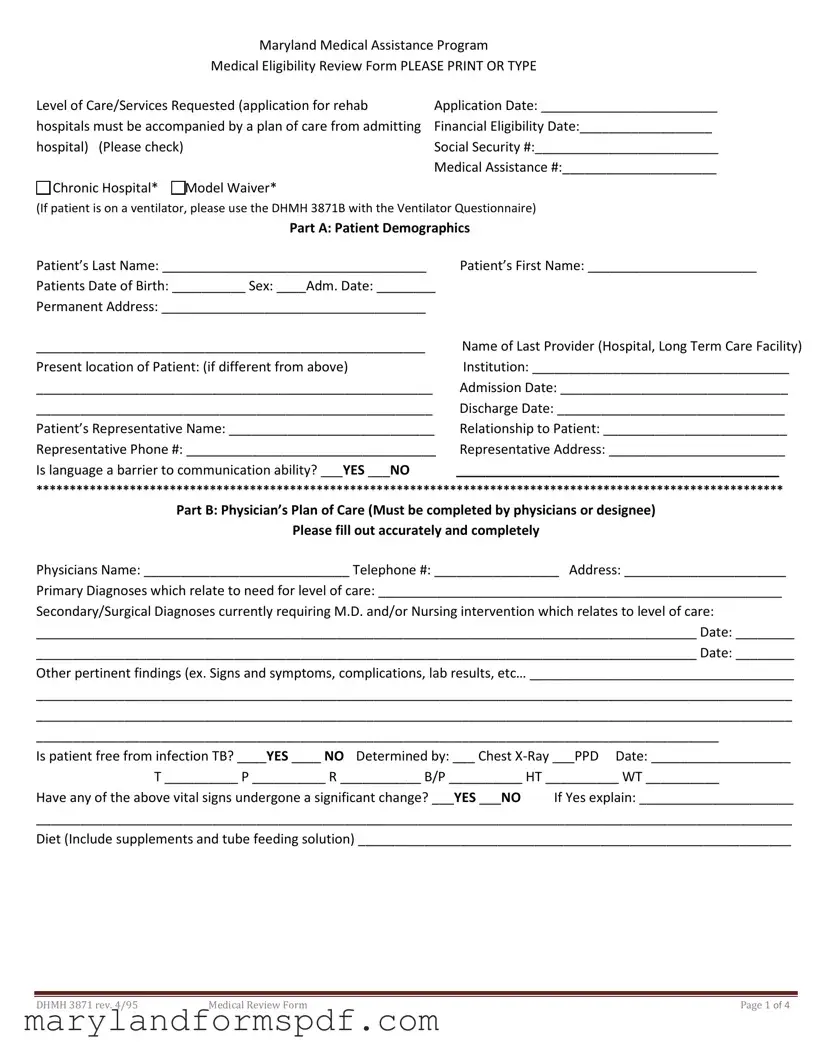
Maryland Medical Assistance Program
Medical Eligibility Review Form PLEASE PRINT OR TYPE
Level of Care/Services Requested (application for rehab |
Application Date: ________________________ |
hospitals must be accompanied by a plan of care from admitting |
Financial Eligibility Date:__________________ |
hospital) (Please check) |
Social Security #:_________________________ |
|
Medical Assistance #:_____________________ |
Chronic Hospital* Model Waiver* |
|
(If patient is on a ventilator, please use the DHMH 3871B with the Ventilator Questionnaire)
Part A: Patient Demographics
Patient’s Last Name: ____________________________________ |
Patient’s First Name: _______________________ |
Patients Date of Birth: __________ Sex: ____Adm. Date: ________ |
|
Permanent Address: ____________________________________ |
|
_____________________________________________________ |
Name of Last Provider (Hospital, Long Term Care Facility) |
Present location of Patient: (if different from above) |
Institution: ___________________________________ |
______________________________________________________ |
Admission Date: _______________________________ |
______________________________________________________ |
Discharge Date: _______________________________ |
Patient’s Representative Name: ____________________________ |
Relationship to Patient: _________________________ |
Representative Phone #: __________________________________ |
Representative Address: ________________________ |
Is language a barrier to communication ability? ___YES ___NO |
____________________________________________ |
****************************************************************************************************************
Part B: Physician’s Plan of Care (Must be completed by physicians or designee)
Please fill out accurately and completely
Physicians Name: ____________________________ Telephone #: _________________ Address: ______________________
Primary Diagnoses which relate to need for level of care: _______________________________________________________
Secondary/Surgical Diagnoses currently requiring M.D. and/or Nursing intervention which relates to level of care:
__________________________________________________________________________________________ Date: ________
__________________________________________________________________________________________ Date: ________
Other pertinent findings (ex. Signs and symptoms, complications, lab results, etc… ____________________________________
_______________________________________________________________________________________________________
_______________________________________________________________________________________________________
_____________________________________________________________________________________________
Is patient free from infection TB? ____YES ____ NO Determined by: ___ Chest
T __________ P __________ R ___________ B/P __________ HT __________ WT __________
Have any of the above vital signs undergone a significant change? ___YES ___NO If Yes explain: _____________________
_______________________________________________________________________________________________________
Diet (Include supplements and tube feeding solution) ___________________________________________________________
|
|
|
DHMH 3871 rev. 4/95 |
Medical Review Form |
Page 1 of 4 |
Patient’s Name: ______________________________
Medication which will be continued:
Medication
Dosage
Frequency
Route
If PRN, avg frequency
Treatment which will be continued: DescriptionFrequencyDuration if Temporary
____ Ventilator: ____________________________________________________________________________________
____ O2 (as well as sats and frequency): _________________________________________________________________
____ Monitor (apnea/bradycardia (A/B), other: ___________________________________________________________
____ Suctioning: ____________________________________________________________________________________
____ Trach Care: ____________________________________________________________________________________
____ IV Line/fluids (indicate central or peripheral): _________________________________________________________
____ Tube Feeding (specify type of tube): ________________________________________________________________
____ Colostomy/ileostomy care: _______________________________________________________________________
____ Catheter/continence device (specify type): __________________________________________________________
____ Frequent labs related to nutrition/needs (describe): ___________________________________________________
____ Decubitus (include size, location, stage, drainage, and signs of infection, also Tx regimen): _____________________
__________________________________________________________________________________________________
____ Other (specify): ________________________________________________________________________________
__________________________________________________________________________________________________
Have any medications or treatments recently been implemented, discontinued, and/or otherwise changed? Explain:
_______________________________________________________________________________________________________
_______________________________________________________________________________________________
Impairments/devices (check all that apply) ___Speech ___Sight ___Hearing ___Other (specify) ______________________
___Devices/Adaptive Equipment ________________________________________________________________________
Active Therapy |
Plan |
Frequency |
Est. Duration |
Goal |
Physical Therapy
Occupational Therapy
Speech Therapy
Respiratory
Others
|
|
|
DHMH 3871 rev. 4/95 |
Medical Review Form |
Page 2 of 4 |

Patient’s Name: 5674
Rehabilitation Potential: ______________________________________________________________________________
Discharge Plan: _____________________________________________________________________________________
*If requesting a level of care for rehab hospital, please answer the following questions:
1.Preexisting condition related to current physical, behavioral and mental functions and deficits: __________________
__________________________________________________________________________________________________
2.Reason for
Is patient comatose? ___YES ___NO if yes skip parts C through E and go directly to part F.
PLEASE NOTE: For other adults applicants, complete parts C and D, skip E. For applicants under age 21, skip parts C and D, complete E.
*************************************************************************************************
|
Part C: Functional Status (Use one of the following codes) |
||
|
(If assistive device (e.g., Wheelchair, Walker) used, note functional ability while using device) |
||
0. |
Little or no difficulty (completely independent |
2. |
Limited physical assistance by caregiver |
|
or setup only is needed |
3. |
Extensive physical assistance by caregiver |
1. |
Supervision/Verbal cuing |
4. |
Total dependence on others |
___ Locomotion (if using adaptive/assistive device, |
___ Dressing |
||
Specify type): _____________________________ |
___ Bathing |
||
___ Transfer bed/chair |
___ Eating |
||
___ Reposition/Bed mobility |
Appetite (Check one): ___ Good ___ Fair ___ Poor |
||
Other functional limitations (describe) ______________________________________________________________________
Incontinence management (Circle applicable choices in each category) (Note status with toileting program and/or continence device, if applicable)
Bladder |
|
|
Bowel |
|
|
|
|
|
0 |
|
|
0 |
|
|
Complete |
||
1 |
|
|
1 |
|
|
Usually |
||
2 |
|
|
2 |
|
|
Occasionally incontinent- accidents 2+ weekly, but not daily |
||
3 |
|
|
3 |
|
|
Frequently incontinent- accidents daily but some control present |
||
4 |
|
|
4 |
|
|
Incontinent- Multiple daily accidents |
||
|
******************************************************************************************************* |
|||||||
|
|
|
|
|
|
|
Part D: Cognitive/Behavioral Status |
|
1. Memory/orientation |
Y=Yes |
N=No |
2. Cognitive skills for daily life decision making and safety (Check one) |
|||||
Yes |
No |
|
|
|
|
|
|
|
___ |
___ |
Can recall after 5 minutes |
___ |
Independent decisions consistent and reasonable |
||||
___ |
___ |
Knows current season |
___ |
Modified/some difficulty in new situations only |
||||
___ |
___ |
Knows own name |
|
|
___ |
Moderately impaired/decisions requires cues/supervision |
||
___ |
___ |
Can recall long past events |
___ |
Severely impaired/rarely or never makes decisions |
||||
___ |
___ |
Knows present location |
|
|
||||
___ |
___ |
Knows family/caretaker |
|
|
||||
3. Communication |
|
0- Always |
|||
Ability to understand others |
|
_____ |
_____ |
_____ |
____ |
Ability to make self understood |
_____ |
_____ |
_____ |
____ |
|
Ability to follow simple commands |
_____ |
_____ |
_____ |
____ |
|
|
|
|
|
|
|
|
|
|
|
|
|
DHMH 3871 rev. 4/95 |
Medical Review Form |
|
|
|
Page 3 of 4 |
Patient’s Name ____________________________________ |
|
|
|
4. Behavior issues (enter one code from A and B in the appropriate column) |
|
|
|
A. Frequency |
B. Easily Altered |
|
|
1= Occasionally |
1= Yes |
|
|
2=Often, but not daily |
2= No |
|
|
3= Daily |
|
|
|
|
|
|
|
|
Description of Problem Behaviors |
A |
B |
|
|
|
|
|
|
|
|
|
|
|
|
5.Most recent
Previous
*******************************************************************************************************
Part E: Functional/Cognitive Status – Pediatric
|
|
Age Appropriate |
|
Functioning Level |
Adaptive Equipment |
|
|
Cognition |
|
|
|
Wheelchair |
|
|
Social Emotional |
|
|
|
Splints/Braces |
|
|
Behavior |
|
|
|
Side Lyer |
|
|
Communications |
|
|
|
Walker |
|
|
Gross Motor Abilities |
|
|
|
Adaptive Seating |
|
|
Fine Motor Abilities |
|
|
|
Communication Devices |
|
|
Feeding |
|
|
|
Other |
|
|
Toileting |
|
|
|
|
|
|
Self Care |
|
|
|
|
|
|
|
Part F: Physician’s Certification for Level of Care |
||||
This patient is certified as in need of the following services (Check One): |
|
|
||||
|
Chronic Hospital |
Model Waiver |
|
|
||
Other information pertinent to need for Long Term Care: _________________________________________________________
Physician’s Signature: ___________________________________________________________ Date: _____________________
Other than physician completing form: ________________________________________________________________________
SignatureTitlePhoneDate
**********************************************************************************************************
This area is for Agent Determination Only. DO NOT write in this area.
|
|
Renewal |
|
___ Medical Eligibility Established |
MD Advisor ___ |
___Medical Eligibility Established |
MD Advisor___ |
___ Medical Eligibility Denied |
|
___ Medical Eligibility Denied |
|
Effective Date: _____________________ |
Effective Date: _____________________ |
||
Type of Service: _________________________________ |
Type of Service: __________________________________ |
||
Certificate Period: From: _____________ To: ___________ |
Certificate Period: From: _____________ To: ___________ |
||
Agent Signature: _________________________________ |
Agent Signature: __________________________________ |
||
Date: ___________________________________________ |
Date: ___________________________________________ |
||
|
|
|
DHMH 3871 rev. 4/95 |
Medical Review Form |
Page 4 of 4 |
File Breakdown
| Fact Name | Description |
|---|---|
| Form Number | DHMH 3871 rev.4/95 |
| Form Title | Maryland Medical Assistance Program Medical Eligibility Review Form |
| Submission Requirement | Application for rehabilitation hospitals must be accompanied by a plan of care from the admitting hospital. |
| Purpose | To review medical eligibility for different levels of care/services within the Maryland Medical Assistance Program. |
| Sections Included | Level of Care/Services Requested, Patient Demographics, Physician’s Plan of Care, Functional Status, Cognitive/Behavioral Status, Functional/Cognitive Status – Pediatric, Physician’s Certification for Level of Care, and Agent Determination. |
| Key Dates | Includes fields for Application date, Financial Eligibility Date, Admission Date, Discharge Date. |
| Governing Law | This form is governed by Maryland state law, specifically regulations related to the Maryland Medical Assistance Program. |
| Accessibility | Questions are included to ensure the form addresses any communication barriers due to language. |
Steps to Filling Out 3871 Maryland Medicaid
Once you receive the 3871 Maryland Medicaid Medical Eligibility Review Form, it's important to fill it out accurately. This document is crucial for determining the appropriate level of care and services required. Careful and clear completion of this form ensures the person in need receives the right medical assistance. Follow the steps below to accurately fill out the form and submit it for processing.
- Begin with Level of Care/Services Requested by checking the correct box that represents the needed service. Make sure to include the application date and the financial eligibility date at the top.
- Enter the Social Security Number and Medical Assistance Number in the designated spaces.
- Proceed to Part A: Patient Demographics. Fill in the patient's last and first names, date of birth, sex, admission date, and the verbal level of care given, along with the name of the utilization control agent.
- Provide the patient's Permanent Address and the name of the last provider, including hospital or long term care facility.
- If the present location of the patient is different from the permanent address, specify the institution's name, admission date, and discharge date.
- Enter the Patient’s Representative information, including name, relationship to the patient, phone number, and address. Indicate if language is a barrier to the patient's ability to communicate.
- Move to Part B: Physician’s Plan of Care, to be completed by a physician. Include the physician’s name, telephone number, and address. Detail the primary and secondary diagnoses that relate to the need for the level of care.
- List out the patient's vital statistics, including whether they are free from infections like TB, and provide details on diet, including any supplements or tube feeding solutions.
- Detail the medications and treatments that will be continued, including dosage, frequency, and route for medications.
- Under Impairments/devices, check all that apply and list any devices or adaptive equipment being used.
- Document the Active Therapy Plan, including physical therapy, occupational therapy, speech therapy, respiratory therapy, and others as applicable.
- Assess the rehabilitation potential and discharge plan, especially if requesting a level of care for rehab hospital usage.
- In Part C, D, and E, as applicable based on the patient's age, fill out sections regarding functional and cognitive status, including information on locomotion, dressing, bathing, eating, cognitive and behavioral status, and for patients under 21, pediatric age-appropriate functioning levels.
- Complete Part F: Physician’s Certification for Level of Care by checking the required services and having the physician sign and date the form.
- Remember, the area marked for Agent Determination is not to be filled by you. Leave this section blank for the reviewing agent.
After completing these steps, review the form for accuracy. Once finished, submit the document as directed by Maryland Medicaid, to ensure a timely and smooth review process. This step is vital for securing necessary medical services.
More About 3871 Maryland Medicaid
What is the purpose of the 3871 Maryland Medicaid Form?
The 3871 Maryland Medicaid Form, also known as the Maryland Medical Assistance Program Medical Eligibility Review Form, is primarily used to review and establish a patient's eligibility for specific levels of medical care under the Maryland Medicaid program. The form captures detailed information about a patient's medical condition, care needs, and treatment plans to determine whether they qualify for services such as nursing facility care, medical day care, rehabilitation hospital services, chronic hospital care, or other waiver programs. By providing comprehensive patient demographics, a physician's plan of care, functional and cognitive status assessments, and a physician's certification for the required level of care, the form plays a crucial role in ensuring that Medicaid recipients receive appropriate and necessary medical services.
Who needs to complete the 3871 Maryland Medicaid Form?
The 3871 Maryland Medicaid Form must be filled out by several parties involved in the care of the patient:
- Patient or Patient's Representative: Part A of the form, which includes patient demographics and information regarding the patient's representative, if applicable, should be filled out by the patient or their designated representative.
- Physician or Designee: Part B, the physician's plan of care, must be accurately and completely filled out by the patient's physician or a designee such as a nurse practitioner or physician assistant who is familiar with the patient's medical condition and care needs.
- Additional Evaluations: Depending on the patient's age and the type of care requested, parts C through E may need to be completed to assess the patient's functional, cognitive, and behavioral status. These sections help in further detailing the patient's eligibility for specific Medicaid services.
How does language ability affect the completion of the form?
The form inquiries about whether language is a barrier to the patient's ability to communicate. This question underscores the importance of ensuring that all patients have the ability to understand and be understood throughout the Medicaid eligibility and service provision processes. If language is identified as a barrier, it may be necessary to provide translation or interpretation services to ensure accurate completion of the form and effective communication about the patient's care needs and options. Addressing language barriers is vital for the equitable access to Medicaid services for all eligible individuals, regardless of their primary language.
What happens after the 3871 Maryland Medicaid Form is submitted?
Once the 3871 Maryland Medicaid Form is submitted, it undergoes a review process by the Maryland Medicaid eligibility team. This process includes:
- An assessment of the detailed information provided in the form to determine the patient’s medical and financial eligibility for Medicaid services.
- Verification of the patient's condition and need for the level of care requested, based on the physician’s recommendations and other supporting documentation provided in the form.
- A determination made by the eligibility team, which may be either approval or denial of the medical eligibility for the requested services. This determination is based on Maryland Medicaid guidelines and the specific needs of the patient as outlined in the submitted form.
Common mistakes
Not checking the correct level of care/services requested: Applicants sometimes fail to select the appropriate box for the level of care they are applying for, such as NF (Nursing Facility), Medical Day Care, Rehab Hospital, Chronic Hospital, or other services. It's crucial to indicate the specific type of medical assistance needed to ensure the application is processed correctly.
Incomplete patient demographics: Skipping or incorrectly filling out any part of the patient's demographic information, like the patient's name, date of birth, sex, permanent address, or social security number, can lead to delays. Accurate details are essential for identity verification and processing the application.
Omitting Admission and Discharge Dates: For patients transferring from another provider, failure to include the admission and discharge dates from the last provider can complicate the review process. These dates help in assessing the continuity of care and the immediate needs of the patient.
Neglecting the physician’s plan of care: The plan of care section must be completed accurately and completely by the physician or their designee. Overlooking this section or providing incomplete information about diagnoses, treatments, and medications can hinder a thorough evaluation of the patient's medical needs.
Incorrect or missing physician information: Every application must include the name, phone number, and address of the physician responsible for the patient's care. This information is crucial for verification and potential follow-up inquiries.
Forgetting to include vital signs information: The form requires details about the patient's temperature, pulse, respiration, blood pressure, height, and weight. Missing information here can affect the assessment of the patient's current health status.
Failure to provide detailed treatment and medication information: Detailed descriptions of ongoing treatments and medications are necessary for a comprehensive review. This includes frequency, dosage, and route for medications, as well as descriptions of any treatments or therapies being continued.
Leaving the functional, cognitive, and behavioral status sections incomplete: These sections help determine the level of assistance the applicant requires. Omitting details or not accurately describing the patient's abilities and needs can lead to an inaccurate determination of eligibility.
Skipping the physician's certification for level of care: The form must be certified by a physician to confirm the need for the requested level of care. Not having this section signed and dated by the physician can result in the application being deemed incomplete.
By paying close attention to these details and ensuring that all sections of the form are completed accurately and thoroughly, applicants can avoid common pitfalls that may delay or affect the outcome of their Maryland Medicaid eligibility assessment.
Documents used along the form
When navigating the complexities of Maryland Medicaid, understanding the auxiliary forms and documents that often accompany the DHMH 3871, or Maryland Medicaid Medical Eligibility Review Form, can provide clarity and streamline the application process. These documents ensure comprehensive review and are vital for accurate determination of eligibility and service levels. Here’s an overview:
- Proof of Income Statements: To verify financial eligibility, applicants must provide recent statements of income. This includes pay stubs, tax returns, or statements from benefits such as Social Security, to name a few.
- Proof of Residency Documents: Essential for establishing the applicant's residency in Maryland. These can include utility bills, a lease agreement, or a driver's license with a current address.
- Identity Verification Documents: A government-issued photo ID, such as a driver's license or passport, is required to confirm the identity of the applicant.
- Social Security Card: A copy of the Social Security card is needed for both the applicant and any dependents.
- Medical Records: Recent medical records that demonstrate the need for the level of care requested. This may include hospital discharge summaries, doctor’s notes, and treatment plans.
- Physician’s Certification: A form completed by a physician certifying the medical necessity for the type of Medicaid services applied for, often required for specialized care levels.
- Power of Attorney or Legal Guardianship Documents: If someone other than the patient is applying on their behalf, these legal documents are necessary to verify their authority to do so.
- Medicaid Renewal Notices: For current recipients, any renewal notices or documentation pertaining to previous Medicaid eligibility and benefits are required to process a renewal application efficiently.
While the DHMH 3871 serves as a foundational document to initiate or renew Medical Assistance, the additional forms and documents play a crucial role in completing the application process. Each piece of documentation aids in painting a full picture of the applicant’s medical needs, financial situation, and eligibility for services, ensuring those in need receive the appropriate care and support. By preparing these materials in advance, applicants can navigate the application process more smoothly and with greater confidence in the comprehensive consideration of their needs.
Similar forms
The 3871 Maryland Medicaid form is similar to several other standard medical and government forms due to its function, structure, and the type of information it collects. Essentially, it gathers comprehensive data regarding a patient's medical eligibility for assistance programs, paralleling other forms in its detailed approach to capturing patient demographics, medical conditions, treatments, and care requirements.
The 3871 form closely resembles the CMS-1500 claim form used by healthcare providers to bill Medicare and most Medicaid state agencies. Both forms are rigorous in collecting patient information, though their applications diverge slightly. The CMS-1500 focuses on billing for services rendered, capturing provider and patient identification details, diagnosis codes, and services provided, which aligns with the Maryland Medicaid form’s collection of similar patient demographics and medical details. Yet, the Maryland form's emphasis on eligibility and level of care differentiation sets it apart, orienting it more towards program admission than direct billing.
Another document sharing similarities is the Social Security Administration’s (SSA) Disability Benefit Application form. This form is designed to assess eligibility for disability benefits, requiring comprehensive personal, medical, and work history information. Both this and the Maryland Medicaid form undertake a meticulous review process of medical conditions and care needs to determine eligibility. They converge on the necessity of thorough medical documentation, including diagnostic information, treatment plans, and functionality assessments, to support the determination process. However, the SSA form uniquely delves into the financial and employment history to evaluate disability benefits, whereas the Maryland Medicaid form focuses on medical care requirements and potential rehabilitation.
Dos and Don'ts
When filling out the Maryland Medicaid 3871 form, ensuring accurate and complete information is critical for the application process. Here are several dos and don'ts to guide you through this process:
- Do print or type the information clearly to prevent any misunderstandings or processing delays caused by illegible handwriting.
- Do check and double-check that all the required sections are filled out, including the patient's demographic details, medical eligibility, and physician's plan of care.
- Do ensure that the application date and financial eligibility date are correctly filled in to avoid processing delays.
- Do accurately report the patient’s Social Security Number and Medical Assistance Number, if available, as these are crucial identifiers in the eligibility process.
- Do fully detail the patient’s medical diagnoses, treatments to be continued, and medications, as incomplete information may lead to an inaccurate assessment of care needs.
- Don't skip the section on the patient's level of care or services requested. Providing a comprehensive plan of care from an admitting hospital, when applicable, is necessary for applications for rehab hospitals.
- Don't leave any fields blank that are applicable to the patient's situation. If a question does not apply, mark it with "N/A" (not applicable) instead of leaving it empty.
- Don't forget to include contact information for the patient’s representative, if one exists, as this individual may need to be contacted for additional information or clarification.
- Don't fail to answer questions related to the patient's impairments or devices used, communication abilities, and rehabilitation potential, as these details are critical for determining the appropriate level of care.
Misconceptions
Common misconceptions about the 3871 Maryland Medicaid form often lead to confusion among individuals attempting to navigate the process of Medical Assistance Program eligibility. These misunderstandings can result in potential delays or denials of much-needed healthcare services. Here are five misconceptions clarified to aid in the comprehension and completion of this vital document.
- The form is solely for nursing facility admissions: While it's true the 3871 form is utilized for determining eligibility for nursing facility care, it's not restricted to just this purpose. It also encompasses eligibility for medical day care, rehab hospitals, chronic hospitals, and other specific waivers, clearly indicating the broad scope of medical services and levels of care it covers.
- Financial information is not relevant: A critical error is the assumption that the form is strictly for determining medical necessity and care level. In reality, it requires both an application date and a financial eligibility date. These sections necessitate an understanding of the individual's financial situation, underscoring the program’s consideration of financial eligibility in parallel to medical needs.
- Personal representation is not necessary: The form not only asks for detailed patient information but also requests the name, relationship, phone number, and address of the patient's representative. This inclusion emphasizes the importance of having an advocate or representative who can assist through the process, showcasing the intricate balance between patient autonomy and the need for supportive advocacy in healthcare decisions.
- Language proficiency is taken for granted: Another oversight is neglecting the section inquiring whether language is a barrier to communication. This question's presence is a clear indicator of the program's commitment to accessibility and inclusivity, ensuring that non-native or limited English proficiency applicants receive appropriate communication assistance throughout their application process.
- Physician’s Plan of Care is secondary: Contrarily, this component is crucial for the approval process. It must be thoroughly filled out by a physician or a registered designee. The detailed plan includes primary and secondary diagnoses, vital signs, dietary needs, medication, and treatment plans, conveying the comprehensive medical overview required to make informed eligibility and care level decisions.
Understanding these misconceptions and their clarifications helps streamline the application process, ensuring individuals seeking assistance through Maryland's Medical Assistance Program are adequately prepared and informed. It highlights the complexity of healthcare assistance programs while underscoring the critical nature of accurate, complete, and clear application submissions.
Key takeaways
Filling out the 3871 Maryland Medicaid Form requires careful attention to detail and accuracy to ensure the proper evaluation of medical eligibility for assistance programs. Here are key takeaways to guide individuals and healthcare providers in completing this form:
- The form supports various levels of care/services requests, including options for Nursing Facility (NF), Medical Day Care, Rehab Hospital, Chronic Hospital, and other specific waivers, highlighting the versatile application for different patient needs.
- Application and financial eligibility dates are critical; they mark the submission time frame and the financial assessment's effective date, which could influence the eligibility determination.
- Comprehensive patient demographics section captures essential information, including the patient’s social security and medical assistance numbers, facilitating a smoother verification process.
- A physician or related professional must complete the Plan of Care section, emphasizing the necessity for a healthcare provider's involvement in accurately detailing the patient's medical condition and care requirements.
- It's imperative to accurately document the primary and secondary diagnoses that necessitate the requested level of care, directly linking the patient's medical needs with the support services sought.
- Detailed medication and ongoing treatment information is required to understand the patient's current health status and care plan continuity, ensuring that the transition to a Medicaid-supported service does not disrupt the patient’s healthcare regimen.
- The form considers functional, cognitive, and behavioral statuses through a series of detailed questions and checklists, underlining Medicaid’s comprehensive approach to assessing patient needs.
- Rehabilitation potential and discharge plans are to be outlined for patients seeking rehab hospital services, demonstrating forward planning and consideration for patient progress.
- Language and communication barriers are acknowledged, ensuring that all patients receive equitable consideration and support regardless of language proficiency.
- Physician certification is required to confirm the necessity of the requested level of care, serving as a crucial endorsement of the application.
- The section reserved for Agent Determination underlines the review and decision-making process that follows the submission of the form, emphasizing its role in the final eligibility determination.
Collectively, these elements ensure the 3871 Maryland Medicaid Form is a comprehensive tool for assessing eligibility for Medicaid's variety of medical assistance programs, underscoring the importance of precision and thoroughness in its completion.
Common PDF Templates
Md Tax Forms - This form is designed for individuals who need to pay taxes not automatically withheld from their income.
Unclaimed Property Maryland - Details about the policy holder’s employer are necessary if the patient has additional insurance coverage.