Maryland Confidential Morbidity Report PDF Template
In the realm of public health, meticulous reporting and data collection are paramount, fostering an environment where infectious diseases are tracked and managed effectively. Within this context, the Maryland Confidential Morbidity Report (DHMH 1140) serves as a critical instrument, designed for the diligent documentation of infectious diseases by physicians and other health care providers, excluding laboratories which are directed to use alternative forms. This report necessitates the disclosure of comprehensive patient information, including personal identifiers, demographics, and details pertinent to the diagnosed condition or disease. The form guides reporters through specifying the onset of the disease, potential hospital admissions, and whether the condition was acquired within the state, alongside suspected sources of infection. Intricately, it delves into determinants such as pregnancy status and exposure to vulnerable populations, highlighting the nuanced aspects of disease transmission and impact. Laboratory results, particularly for viral hepatitis and HIV/AIDS, are rigorously detailed, advocating for a clear understanding of the patient’s health status. Furthermore, additional case information sections emphasize the importance of recognizing and reporting on sexually transmitted infections (STIs) and tuberculosis, underscoring the breadth of conditions that significantly concern public health officials. Through its structured inquiries, the form demonstrates a methodical approach to disease reporting, vital for the effective monitoring, control, and prevention of infectious diseases within Maryland. The inherent detail and comprehensive scope of the Maryland Confidential Morbidity Report affirm its significance in the concerted effort to safeguard public health.
Maryland Confidential Morbidity Report Sample
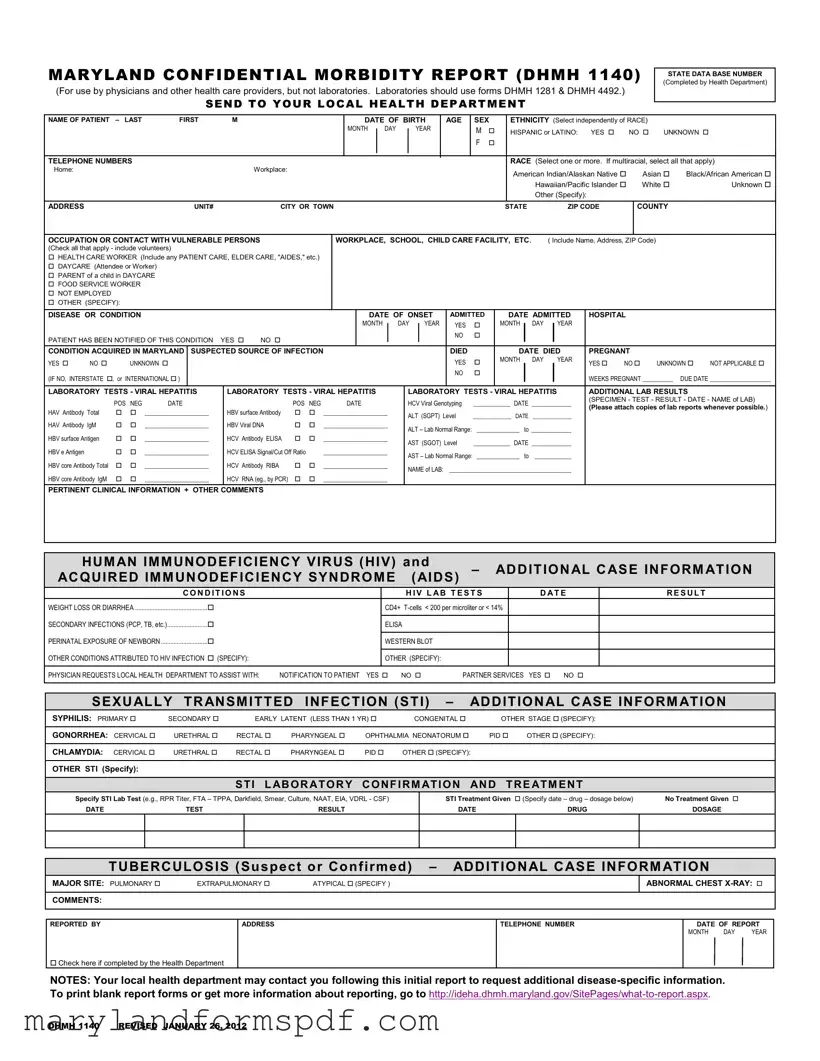
MARYLAND CONFIDENTIAL MORBIDITY REPORT (DHMH 1140)
(For use by physicians and other health care providers, but not laboratories. Laboratories should use forms DHMH 1281 & DHMH 4492.)
SEND TO YOUR LOCAL HEALTH DEPARTMENT
STATE DATA BASE NUMBER (Completed by Health Department)
NAME OF PATIENT |
– LAST |
FIRST |
|
M |
|
|
|
|
|
|
DATE OF BIRTH |
|
AGE |
SEX |
|
ETHNICITY (Select independently of RACE) |
|
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
MONTH |
|
DAY |
|
|
YEAR |
|
|
M |
|
|
HISPANIC or LATINO: |
YES |
|
NO |
UNKNOWN |
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TELEPHONE NUMBERS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
RACE (Select one or more. If multiracial, select all that apply) |
|||||||||||||||||
Home: |
|
|
|
|
|
|
|
Workplace: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
American Indian/Alaskan Native |
|
Asian |
Black/African American |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Hawaiian/Pacific Islander |
|
White |
|
Unknown |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Other (Specify): |
|
|
|
|
|
|
|
|||
ADDRESS |
|
|
|
|
UNIT# |
|
|
CITY OR TOWN |
|
|
|
|
|
|
|
|
|
|
|
STATE |
|
|
ZIP CODE |
|
|
COUNTY |
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
OCCUPATION OR CONTACT WITH VULNERABLE PERSONS |
|
|
|
WORKPLACE, SCHOOL, CHILD CARE FACILITY, ETC. |
|
( Include Name, Address, ZIP Code) |
|
|
|
|||||||||||||||||||||||||||||||||
(Check all that apply - include volunteers) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
HEALTH CARE WORKER (Include any PATIENT CARE, ELDER CARE, "AIDES," etc.) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
DAYCARE (Attendee or Worker) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
PARENT of a child in DAYCARE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
FOOD SERVICE WORKER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
NOT EMPLOYED |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
OTHER (SPECIFY): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
DISEASE OR CONDITION |
|
|
|
|
|
|
|
|
|
|
DATE OF ONSET |
ADMITTED |
|
|
DATE ADMITTED |
|
HOSPITAL |
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MONTH |
|
|
DAY |
|
YEAR |
YES |
|
|
MONTH |
|
|
DAY |
|
YEAR |
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
PATIENT HAS BEEN NOTIFIED OF THIS CONDITION |
YES |
NO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
CONDITION ACQUIRED IN MARYLAND |
SUSPECTED SOURCE OF INFECTION |
|
|
|
|
|
|
|
|
|
|
|
|
|
DIED |
|
|
|
|
DATE DIED |
|
PREGNANT |
|
|
|
|||||||||||||||||
YES |
NO |
|
UNKNOWN |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
YES |
|
|
MONTH |
DAY |
|
YEAR |
|
YES |
NO |
UNKNOWN |
NOT APPLICABLE |
||||||||
(IF NO, INTERSTATE , or INTERNATIONAL ) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NO |
|
|
|
|
|
|
|
|
|
|
|
WEEKS PREGNANT __________ |
DUE DATE ____________________ |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LABORATORY TESTS - VIRAL HEPATITIS |
|
LABORATORY TESTS - VIRAL HEPATITIS |
|
|
|
|
LABORATORY TESTS - VIRAL HEPATITIS |
|
ADDITIONAL LAB RESULTS |
|
||||||||||||||||||||||||||||||||
|
|
POS |
NEG |
DATE |
|
|
|
POS |
NEG |
|
|
DATE |
|
|
|
|
HCV Viral Genotyping |
____________ |
DATE _____________ |
|
(SPECIMEN - TEST - RESULT - DATE - NAME of LAB) |
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
(Please attach copies of lab reports whenever possible.) |
||||||||||||||||||||||||||||||
HAV Antibody Total |
|
|
_____________________ |
|
HBV surface Antibody |
|
|
_____________________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
ALT (SGPT) Level |
______________ |
DATE |
______________ |
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
HAV Antibody IgM |
|
|
_____________________ |
|
HBV Viral DNA |
|
|
_____________________ |
|
|
|
ALT – Lab Normal Range: |
______________ to _____________ |
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
HBV surface Antigen |
|
|
_____________________ |
|
HCV Antibody ELISA |
|
|
_____________________ |
|
|
|
AST (SGOT) Level |
____________ |
DATE _____________ |
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
HBV e Antigen |
|
|
|
_____________________ |
|
HCV ELISA Signal/Cut Off Ratio |
|
_____________________ |
|
|
|
AST – Lab Normal Range: ______________ to |
____________ |
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
HBV core Antibody Total |
|
|
_____________________ |
|
HCV Antibody RIBA |
|
|
_____________________ |
|
|
|
NAME of LAB: |
________________________________________ |
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
HBV core Antibody IgM |
|
|
_____________________ |
|
HCV RNA (eg., by PCR) |
|
|
_____________________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
PERTINENT CLINICAL INFORMATION + OTHER COMMENTS
|
HUMAN IMMUNODEFICIENCY VIRUS (HIV) and |
– |
ADDITIONAL CASE INFORMATION |
||||
|
ACQUIRED IMMUNODEFICIENCY SYNDROME |
(AIDS) |
|||||
|
CON D IT IO NS |
|
H IV L AB T EST S |
|
D AT E |
RESULT |
|
|
WEIGHT LOSS OR DIARRHEA ............................................. |
CD4+ |
|
|
|||
|
SECONDARY INFECTIONS (PCP, TB, etc.)......................... |
|
|
|
|
|
|
|
ELISA |
|
|
|
|
|
|
|
PERINATAL EXPOSURE OF NEWBORN ............................. |
|
|
|
|
|
|
|
WESTERN BLOT |
|
|
|
|
||
|
OTHER CONDITIONS ATTRIBUTED TO HIV INFECTION (SPECIFY): |
|
|
|
|
|
|
|
OTHER (SPECIFY): |
|
|
|
|
||
PHYSICIAN REQUESTS LOCAL HEALTH DEPARTMENT TO ASSIST WITH: NOTIFICATION TO PATIENT YES NO PARTNER SERVICES YES NO
SEXUALLY TRANSMITTED INFECTION (STI) – |
ADDITIONAL CASE INFORMATION |
|||||
SYPHILIS: PRIMARY |
SECONDARY |
EARLY LATENT (LESS THAN 1 YR) |
CONGENITAL |
OTHER STAGE (SPECIFY): |
||
|
|
|
|
|
|
|
GONORRHEA: CERVICAL |
URETHRAL |
RECTAL |
PHARYNGEAL |
OPHTHALMIA NEONATORUM |
PID OTHER (SPECIFY): |
|
|
|
|
|
|
|
|
CHLAMYDIA: CERVICAL |
URETHRAL |
RECTAL |
PHARYNGEAL |
PID |
OTHER (SPECIFY): |
|
|
|
|
|
|
|
|
OTHER STI (Specify): |
|
|
|
|
|
|
STI LABORATORY CONFIRMATION AND TREATMENT
Specify STI Lab Test (e.g., RPR Titer, FTA – TPPA, Darkfield, Smear, Culture, NAAT, EIA, VDRL - CSF)
DATE |
TEST |
RESULT |
STI Treatment Given (Specify date – drug – dosage below) |
No Treatment Given |
|
DATE |
DRUG |
DOSAGE |
TUBERCULOSIS (Suspect or Confirmed) – ADDITIONAL CASE INFORMATION
MAJOR SITE: PULMONARY |
EXTRAPULMONARY |
ATYPICAL (SPECIFY ) |
ABNORMAL CHEST
COMMENTS:
REPORTED BY
ADDRESS
TELEPHONE NUMBER
DATE OF REPORT
MONTH DAY YEAR
Check here if completed by the Health Department
NOTES: Your local health department may contact you following this initial report to request additional
DHMH 1140 REVISED JANUARY 26, 2012
File Breakdown
| Fact Name | Detail |
|---|---|
| Form Title | Maryland Confidential Morbidity Report (DHMH 1140) |
| Intended Users | Physicians and other health care providers (excluding laboratories) |
| Alternative Forms for Laboratories | DHMH 1281 & DHMH 4492 |
| Submission Destination | Local Health Department |
| Key Information Captured | Patient demographics, disease or condition, suspected source of infection, pregnancy status, laboratory tests, HIV and AIDS conditions, STI information |
| Source for Reporting Guidelines | Maryland Department of Health Information on Reporting |
Steps to Filling Out Maryland Confidential Morbidity Report
Once the Maryland Confidential Morbidity Report form is completed, it must be sent to the local health department. This crucial step ensures proper handling of the information, allows for timely follow-up, and aids in the management and control of diseases within the community. Careful attention to detail and accuracy in filling out the form is paramount to ensure all relevant information is communicated effectively.
- Start by entering the patient's full name, with the last name first, followed by the first name and middle initial.
- Fill in the date of birth using the format month/day/year, then enter the patient's age and sex.
- Select the patient's ethnicity; choose yes, no, or unknown for Hispanic or Latino.
- Indicate the patient's race. Check all that apply. If the race is not listed, select "Other" and specify.
- Provide the telephone numbers for the patient, including home and workplace contacts.
- Enter the complete home address, including the unit number, city or town, state, ZIP code, and county.
- Detail the patient's occupation or any contact with vulnerable persons. Check all boxes that apply and specify if the occupation is other than the options provided.
- Indicate the disease or condition being reported, the date of onset, and if the patient was admitted to a hospital, including the admit date.
- Confirm if the patient has been notified of this condition with a yes or no.
- Mark if the condition was acquired in Maryland, the suspected source of infection, and if applicable, details regarding the patient's pregnancy status.
- For viral hepatitis laboratory tests, check the appropriate test(s) performed, result (positive/negative), and date. Attach copies of lab reports if available.
- Under the section for HIV and AIDS conditions, mark all conditions that apply and provide specific lab test results, including the date and outcome.
- If requesting the local health department's assistance with patient notification or partner services, check the appropriate box.
- For additional case information on sexually transmitted infections (STIs) like syphilis, gonorrhea, chlamydia, or others, specify the condition, laboratory confirmation, and treatment details.
- If the report involves tuberculosis, specify the major site of the disease, and if there were any abnormal chest X-ray findings, provide comments.
- Complete the reporting section with the reporter's name, address, telephone number, and the date of the report. If completed by the health department, check the indicated box.
After submitting the Maryland Confidential Morbidity Report to the local health department, they may reach out for additional information. For further details on disease reporting or to obtain blank report forms, visit the official Maryland Department of Health website.
More About Maryland Confidential Morbidity Report
What is the purpose of the Maryland Confidential Morbidity Report form (DHMH 1140)?
The Maryland Confidential Morbidity Report form, or DHMH 1140, is specifically designed for use by physicians and other healthcare providers to report specific diseases or conditions to the local health department. The intent behind this form is to facilitate the timely communication of information about notifiable diseases to public health officials. By doing so, it allows for a swift public health response, including investigation, control of disease spread, and the implementation of prevention strategies. Unlike this form, laboratories have designated forms, namely DHMH 1281 and DHMH 4492, for their reporting purposes.
Who is required to complete and submit the Maryland Confidential Morbidity Report form?
This form is mandatory for physicians and other healthcare providers when they identify diseases or conditions in a patient that are of public health importance and thus, are reportable under Maryland law. It is not intended for laboratory use. Laboratories have their own forms (DHMH 1281 & DHMH 4492) for reporting. The responsibility of healthcare providers includes not only diagnosing and treating patients but also playing a crucial role in the surveillance and control of communicable diseases by reporting them to public health authorities.
What kind of information is requested on the form?
The form requests detailed patient information, including but not limited to:
- Full name and contact information
- Date of birth, age, sex, and ethnicity
- Race, occupation and contact with vulnerable populations
- Specific details about the disease or condition, including the date of onset, if the patient was admitted to a hospital, and if the condition was acquired in Maryland
- Laboratory tests conducted, including results for viral hepatitis and HIV/AIDS if relevant
- Other pertinent clinical information and any additional comments
It is essential that healthcare providers supply as much accurate and complete information as possible to aid public health officials in their efforts to track and manage the reported conditions.
How is patient confidentiality maintained when submitting this form?
Patient confidentiality is of utmost importance. The Maryland Confidential Morbidity Report form is designed with strict adherence to confidentiality laws and protocols to protect patient information. The information collected is used solely for public health purposes, such as disease tracking, management, and prevention efforts. It is securely stored and only accessible by authorized public health personnel. Healthcare providers and public health officials are both bound by confidentiality obligations to ensure that sensitive information is handled with the highest degree of care and security.
Where should the completed Maryland Confidential Morbidity Report form be sent?
Once completed, the form should be promptly sent to your local health department. Immediate reporting ensures that necessary public health actions can be taken without undue delay. For contact information and to determine the specific office to which the form should be sent, healthcare providers can visit the Maryland Department of Health's website or directly contact their local health department.
Can the form be accessed and submitted electronically?
As of the latest information available, the form should be completed and then sent to the appropriate local health department. For the most current information regarding the availability of electronic submission or to access printable forms, healthcare providers are encouraged to visit the Maryland Department of Health's official website or contact their local health department directly. The deployment of electronic health reporting systems can vary across jurisdictions, and thus, checking with local health authorities is advisable for the latest submission protocols.
Common mistakes
Filling out the Maryland Confidential Morbidity Report (DHMH 1140) is a crucial step for physicians and other healthcare providers to report certain diseases and conditions to the local health department. However, errors can occur during the completion of this form, which may lead to discrepancies or delays in the reporting process. Here are four common mistakes:
- Incorrect or Incomplete Patient Information:
- Not fully completing the patient's name, including the last and first name, or omitting the middle initial when it is available.
- Failing to provide the full date of birth, including the month, day, and year, which is crucial for patient identification and disease tracking.
- Leaving the ethnicity and race sections blank or inaccurately filled. Both fields are independent and should be completed based on the patient's self-identification, which helps in understanding the disease's impact on different populations.
- Misreporting of Disease or Condition Details:
- Incorrect or missing date of onset of the disease or condition, which is vital for tracking the disease's progression and initiating timely public health interventions.
- Omitting the suspected source of infection or incorrectly identifying the condition as acquired in Maryland when it was not.
- Lab Test Results Reporting Errors:
- Not attaching copies of lab reports when possible, which can provide a comprehensive view of the patient's condition and are essential for a detailed review and action.
- Incorrectly marking lab test results as positive or negative without verifying the laboratory's final report, leading to potential misreporting of the disease's presence.
- Incomplete Reporting on Special Conditions:
- Forgetting to indicate if the patient is pregnant, which is crucial information that affects the course of treatment and monitoring.
- Omitting the number of weeks pregnant and the due date for pregnant patients, which are necessary for appropriate care and follow-up.
By avoiding these common mistakes, healthcare providers can ensure their reports are accurate and complete, ultimately aiding in the effective monitoring and control of diseases within Maryland.
Documents used along the form
When medical professionals submit the Maryland Confidential Morbidity Report form, it's often just the beginning of a thorough reporting process. Various other documents may be required to comprehensively document a patient's health status and ensure that public health officials have all the necessary information. These additional forms and documents support the initial report by providing more detailed data or covering related areas of concern.
- Notice of Privacy Practices: This document is crucial for informing patients about how their health information will be used and shared. It outlines the practices to protect patient confidentiality while complying with public health reporting requirements.
- Laboratory Request Form: Often accompanies the morbidity report when additional tests are necessary to confirm a diagnosis. It specifies the tests required and provides details about the patient and specimen collection.
- Patient Consent Form for Disclosure of Health Information: This form is important when health information needs to be shared with other entities. It obtains the patient's permission to disclose their health details for treatment, payment, or healthcare operations.
- Physician’s Report to Public Health Department: Used by doctors to report notifiable diseases, this document may include more detailed clinical information and the physician's observations beyond what is captured in the morbidity report.
- Immunization Record: In cases where vaccine-preventable diseases are reported, an updated immunization record helps public health officials understand a patient's vaccine history and potential immunity.
- Disease Investigation Questionnaire: For certain contagious or high-risk diseases, detailed questionnaires help trace contacts, sources of infection, and potential outbreaks. These forms are crucial for effective disease control and prevention efforts.
- Death Certificate: In the unfortunate event of a patient's death, this legal document records the cause of death, among other details. For diseases with significant morbidity and mortality, death certificates provide vital statistical information.
Compiling these documents alongside the Maryland Confidential Morbidity Report form offers a multidimensional view of public health concerns. This comprehensive approach allows for better management of diseases and conditions, ultimately contributing to the health and safety of the community.
Similar forms
The Maryland Confidential Morbidity Report form is similar to various other reporting documents used within the healthcare and public health sectors. These forms share common features including the detailed collection of patient data, the purpose for which they are used—such as tracking and managing diseases—and a structured format for submitting this information to relevant authorities or health departments. Below are examples of documents that have notable similarities to the Maryland Confidential Morbidity Report form:
Healthcare Associated Infections (HAI) Reporting Forms:
- Similarity in Purpose: Both the Maryland Confidential Morbidity Report form and HAI Reporting Forms are used to track illnesses. While the Maryland form tracks a wide range of conditions, HAI forms are specifically designed for infections acquired in healthcare settings. Such tracking helps in monitoring outbreaks and understanding infection control challenges.
- Data Collection: These forms collect detailed patient information including demographics, clinical data, and the outcome of the illness. This assists health departments in identifying patterns and taking appropriate public health actions.
- Reporting Structure: Both forms include sections for laboratory results, which are crucial for confirming diagnoses. They also have fields for reporting the date of symptom onset and, if applicable, hospital admission, reflecting their role in timely and accurate disease surveillance.
Immunization Reporting Forms:
- Similarity in Data Elements: Immunization Reporting Forms and the Maryland Confidential Morbidity Report share similarities in the type of patient data collected, such as name, date of birth, and contact information. This fundamental patient information is vital for tracking health events within populations.
- Public Health Objective: Both forms serve public health objectives—monitoring disease prevalence and vaccine coverage, respectively. This information is crucial for identifying at-risk populations and enhancing community health interventions.
Usage by Health Care Providers: Similar to the Maryland form, Immunization Reporting Forms are also filled out by healthcare providers. This underscores the role of healthcare personnel in disease surveillance and prevention efforts within their communities.
Sexually Transmitted Infections (STI) Reporting Forms:
- Targeted Health Conditions: Like the Maryland Confidential Morbidity Report, STI Reporting Forms focus on specific health conditions. In this case, the conditions are sexually transmitted infections. Both forms play a critical role in disease tracking and identifying trends over time.
- Confidentiality: A key feature of both documents is their emphasis on confidentiality, given the sensitive nature of the information they collect. This ensures patient privacy while allowing for the effective monitoring of public health concerns.
- Integration with Public Health Initiatives: By reporting detailed case information, these forms assist in targeted public health initiatives and resource allocation—for example, in STI prevention programs or emergency response to outbreaks.
Each of these documents, while tailored to their specific health monitoring purposes, parallels the Maryland Confidential Morbidity Report in their combined efforts to compile comprehensive health data. This data serves as the foundation for informed public health strategies and interventions, ultimately aiming to improve population health outcomes.
Dos and Don'ts
When filling out the Maryland Confidential Morbidity Report form, it's crucial to provide accurate and complete information to ensure the health and safety of Maryland residents. Here are six do's and don'ts to guide you through the process:
- Do ensure that all patient information is filled out accurately, including the patient's full name, date of birth, age, sex, ethnicity, race, and contact information. This information is vital for identifying the patient and ensuring proper follow-up.
- Do select the correct disease or condition being reported, and be precise about the date of onset, date of diagnosis, and whether the patient has been admitted to a hospital. Accurate reporting of this information helps in understanding the spread and impact of diseases.
- Do report if the condition was acquired in Maryland or elsewhere, as this information is crucial for tracking disease origin and preventing further spread within the state.
- Don't leave laboratory test sections incomplete. Provide all available results of relevant tests, including details like the specimen, test performed, result, and date. If the form requests specific laboratory tests such as Viral Hepatitis or HIV lab tests, attach copies of lab reports whenever possible.
- Don't forget to mark if the patient has been notified of the condition, if they are pregnant, and the suspected source of infection if known. These details are essential for managing public health responses and providing targeted support to affected individuals.
- Don't overlook sections that may seem not immediately relevant, such as occupation, contact with vulnerable persons, or additional case information for other conditions like HIV/AIDS or STIs. This comprehensive approach helps public health professionals understand the broader context of each case.
Remember, the information you provide on the Maryland Confidential Morbidity Report form helps public health officials monitor, manage, and mitigate the spread of diseases in Maryland efficiently. Always double-check your entries for accuracy and completeness before sending the report to your local health department.
Misconceptions
Many misconceptions surround the Maryland Confidential Morbidity Report form, which could affect its use and the reporting process. Clearing up these misconceptions is crucial for accurate and efficient reporting of medical conditions to help with public health monitoring and intervention efforts. Here are five common misconceptions:
- Intended for Laboratory Use: Despite what some may believe, the Maryland Confidential Morbidity Report (DHMH 1140) is not for laboratory use. Laboratories should use forms DHMH 1281 & DHMH 4492. Instead, DHMH 1140 is intended for physicians and other healthcare providers to report certain conditions.
- Public Submission: It's a misconception that the general public can submit this form. In reality, the form is designed specifically for use by physicians and healthcare providers to report to their local health department, ensuring that sensitive health information is handled by professionals.
- Includes Extensive Personal Information: While the form requires some personal information to adequately report health conditions, it does not intrude excessively into personal privacy. Necessary fields include name, date of birth, and contact information, focusing on the purpose of public health safety rather than personal scrutiny.
- Reporting is Optional: Some may misunderstand the nature of reporting with this form, thinking it's optional. However, reporting certain diseases or conditions using the Maryland Confidential Morbidity Report is a legal requirement for healthcare providers to aid in monitoring and controlling public health issues.
- Complex Submission Process: Though it might seem daunting, the submission process for this report has been streamlined to be as straightforward as possible. Healthcare providers must simply complete the form and send it to their local health department, which can then take further steps as needed.
Correcting these misconceptions is essential for the adequate reporting and management of health conditions in Maryland, ensuring that public health authorities have the information they need to protect the community. By understanding the actual requirements and uses of the Maryland Confidential Morbidity Report, healthcare providers can fulfill their reporting duties more effectively and efficiently.
Key takeaways
When filling out the Maryland Confidential Morbidity Report form, it’s important to keep several key takeaways in mind to ensure accurate and effective reporting. These takeaways are vital for health care providers who are tasked with reporting various health conditions to the local health department.
- Intended Users: This form is specifically designed for use by physicians and other health care providers. Laboratories have separate forms (DHMH 1281 & DHMH 4492) designated for their reporting.
- Comprehensive Patient Information: The form requires detailed patient information including name, date of birth, sex, ethnicity, race, contact numbers, and address. It is crucial to fill out this section completely and accurately.
- Employment and Vulnerable Contact Information: Information regarding the patient's occupation or any contact with vulnerable persons is necessary. This includes specifying if the patient is a health care worker, involved in daycare (either as a worker or a parent of a child in daycare), a food service worker, etc.
- Disease or Condition Reporting: The form requests specifics about the disease or condition being reported, including the date of onset, hospital admission details, and the patient's notification of their condition.
- Pregnancy Information: If applicable, information on whether the patient is pregnant, the number of weeks pregnant, and the due date is required, highlighting the need for careful consideration in managing and reporting conditions affecting pregnant individuals.
- Laboratory Tests: A detailed section on various laboratory tests is included, especially for reporting viral hepatitis. This emphasizes the importance of attaching laboratory reports whenever possible to provide a comprehensive view of the patient's condition.
- Additional Information: The form allows space for pertinent clinical information and other comments, which can include symptoms, secondary infections, and conditions attributed to HIV/AIDS, along with specific requests for assistance from the local health department in notifying the patient or partner services.
- Reporting Sexually Transmitted Infections (STI) and Tuberculosis (TB): Detailed sections for reporting STIs and TB are present, indicating the necessity of specifying laboratory confirmation, treatment given, and major sites affected for TB.
The Maryland Confidential Morbidity Report form is a critical tool in tracking and managing the spread of diseases within the state. By diligently completing the form, health care providers play a significant role in public health surveillance and intervention efforts.
Common PDF Templates
Maryland Tax Form - Includes provisions for reporting changes due to acquisitions, consolidations, or other significant events.
Maryland Lottery Winner Anonymous - Guides through the appeal process for those whose applications for a Maryland Lottery license have been denied.
Maryland Sales and Use Tax - A legal form in Maryland that allows businesses to not pay sales tax on items bought for resale.