Maryland State Claim PDF Template
Filing a claim with the State of Maryland for health-related expenses can seem daunting, but understanding the essentials of the Maryland State Employees Health Claim Form can simplify the process. Designed exclusively for members of the State Employees Health Plan, including those enrolled in PPO, POS, and EPO plans, this form is a crucial step for employees who seek reimbursement for services received from non-participating providers. Key sections of the form require detailed personal and patient information, such as legal names, membership and group numbers, and addresses, alongside health and insurance details that encompass questions about the nature of the treatment, its relation to any accidents or work-related injuries, and any other insurance coverages. Additionally, the form outlines specific documentation needed for processing, including itemized bills with comprehensive details like the provider’s diagnosis, dates of service, and charges for each service, translating and converting details for services obtained abroad if necessary. The guidance notes remind claimants to attach all necessary documentation, like bills on the provider’s letterhead and any relevant payment statements from other insurers, which are termed in the form as “Explanation of Benefits” or similar. Furthermore, to ensure fidelity, it includes a stern warning about the legal repercussions of submitting false or fraudulent claims, reinforcing the importance of accuracy and honesty in completing the form. To complete the submission, the subscriber's signature is mandatory, serving as a testimony to the veracity of the information provided and authorizing the release of medical information necessary for the claim's evaluation. CareFirst BlueCross BlueShield, as the processor for these claims, emphasizes the necessity of following the form’s instructions meticulously to ensure a smooth claim process, offering additional guidance through their Member Service and online resources.
Maryland State Claim Sample
Do not write in this space
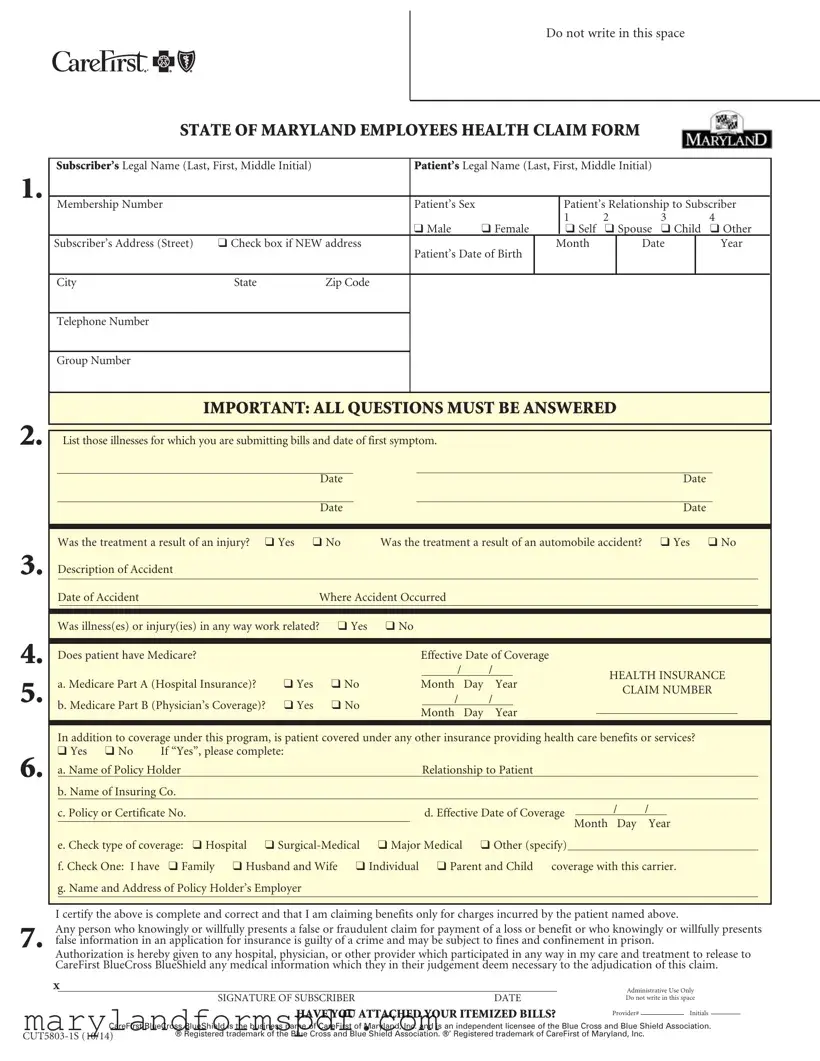
STATE OF MARYLAND EMPLOYEES HEALTH CLAIM FORM
1.
2.
3.
4.
5.
6.
7.
Subscriber’s Legal Name (Last, First, Middle Initial) |
|
Patient’s Legal Name (Last, First, Middle Initial) |
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|||
Membership Number |
|
|
Patient’s Sex |
|
|
Patient’s Relationship to Subscriber |
|
|||||
|
|
|
|
|
|
1 |
2 |
|
3 |
|
4 |
|
|
|
|
q Male |
q Female |
|
q Self |
q Spouse |
q Child |
q Other |
|
||
Subscriber’s Address (Street) |
q Check box if NEW address |
Patient’s Date of Birth |
Month |
|
Date |
|
Year |
|
||||
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
State |
Zip Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Telephone Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Group Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
IMPORTANT: ALL QUESTIONS MUST BE ANSWERED
|
|
List those illnesses for which you are submitting bills and date of first symptom. |
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date |
|
|
|
|
|
|
|
|
|
|
|
Date |
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
Date |
|
|
|
|
|
|
|
|
|
|
|
Date |
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
Was the treatment a result of an injury? |
q Yes q No |
Was the treatment a result of an automobile accident? |
q Yes q No |
|
|||||||||||||||||
|
Description of Accident |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Date of Accident |
|
Where Accident Occurred |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Was illness(es) or injury(ies) in any way work related? |
q Yes |
q No |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Does patient have Medicare? |
|
|
|
|
|
Effective Date of Coverage |
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
/ |
|
/ |
|
|
|
HEALTH INSURANCE |
|
|||||||
|
a. Medicare Part A (Hospital Insurance)? |
q Yes |
q No |
|
|
Month |
Day |
Year |
|
|
|
|||||||||||
|
|
|
|
|
CLAIM NUMBER |
|
||||||||||||||||
|
|
|
|
|
|
|
|
/ |
|
/ |
|
|
|
|
||||||||
|
b. Medicare Part B (Physician’s Coverage)? q Yes |
q No |
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
Month |
Day |
Year |
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
In addition to coverage under this program, is patient covered under any other insurance providing health care benefits or services? |
|
||||||||||||||||||||
|
q Yes q No |
If “Yes”, please complete: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
a. Name of Policy Holder |
|
|
|
|
|
|
Relationship to Patient |
|
|
|
|
|
|
|
|
|
|||||
|
b. Name of Insuring Co. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
c. Policy or Certificate No. |
|
|
|
|
|
|
d. Effective Date of Coverage |
|
/ |
/ |
|
|
|
|
|
||||||
|
|
|
|
|
|
|
Month Day |
Year |
|
|||||||||||||
|
e. Check type of coverage: q Hospital |
q |
q Major Medical |
q Other (specify) |
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
f. Check One: I have |
q Family q Husband and Wife q Individual q Parent and Child coverage with this carrier. |
|
|||||||||||||||||||
|
g. Name and Address of Policy Holder’s Employer |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
I certify the above is complete and correct and that I am claiming benefits only for charges incurred by the patient named above.
Any person who knowingly or willfully presents a false or fraudulent claim for payment of a loss or benefit or who knowingly or willfully presents false information in an application for insurance is guilty of a crime and may be subject to fines and confinement in prison.
Authorization is hereby given to any hospital, physician, or other provider which participated in any way in my care and treatment to release to CareFirst BlueCross BlueShield any medical information which they in their judgement deem necessary to the adjudication of this claim.
X
SIGNATURE OF SUBSCRIBER |
DATE |
HAVE YOU ATTACHED YOUR ITEMIZED BILLS?
Administrative Use Only
Do not write in this space
Provider# |
|
Initials |
CareFirst BlueCross BlueShield is the business name of CareFirst of Maryland, Inc. and is an independent licensee of the Blue Cross and Blue Shield Association.
® Registered trademark of the Blue Cross and Blue Shield Association. ®’ Registered trademark of CareFirst of Maryland, Inc.

Mail Administrator
P.O. Box 14115
Lexington, KY
STATE OF MARYLAND EMPLOYEES HEALTH CLAIM FORM
This form is to be used only by members of the State Employees Health Plan to file PPO, POS and EPO claims. While participating providers will bill CareFirst BlueCross BlueShield for services rendered, you may have claims to file yourself if you see
• A copy of the bill on the provider’s letterhead stationary
IN ORDER FOR YOUR CLAIMS TO BE PROCESSED, THE FOLLOWING INFORMATION MUST BE SUBMITTED
The bill must include:
Provider’s full name, degree, address, phone # and CareFirst BlueCross BlueShield provider number if available.
Patient’s full name
Descriptions of each service or supply
Date of which each service was provided
The provider’s diagnosis, or patient’s chief complaint
The amount charged by the provider for each service provided
Bills in foreign language should be translated to English, foreign currency should be converted to American dollars
Original bills and receipts required for all services
Keep a copy of your bills and claim for your records
Provider’s signature is required
•A completed claim form. Please be sure to accurately complete all sections of the claim form. Always use one claim form per patient.
•When another insurance carrier (including Medicare) is paying your claim first, please submit a copy of their payment statement with your claim. These statements are sometimes called “Explanation of Benefits,” “Summary of Benefits,” “Explanation of Medicare Benefits.”
BILLS FOR THE FOLLOWING SERVICES SHOULD INCLUDE THIS ADDITIONAL INFORMATION
Office Visits: |
Type of visit (brief, intermediate, extended, etc.) |
Private Duty Nursing: |
Dates and shifts worked, amount charged for each shift, prescribing Doctor’s name and degree, |
|
and registration # of nurse. |
Durable Medical Equipment: |
Include the full purchase price of any rented equipment. A letter of medical necessity from your |
(wheelchair, respirator, oxygen, etc.) |
physician must be submitted with the claim. |
Type of |
|
Blood Charges: |
Include the number of pints received, charges for each, and the number of pints replaced by |
|
donors. Indicate whether bill is for whole blood, plasma or derivatives. |
General Anesthesia: |
The length of time (in minutes) the patient was under general anesthesia must appear on the bill. |
Accidental Injury Claims: |
Must indicate the date on which the accident occurred. |
Members of the Preferred Provider Option (PPO), Exclusive Provider Organization (EPO) and Point of Service (POS) – Note: Must have pre- authorization on file after the sixth visit for outpatient physical therapy, occupational therapy and after first visit for speech therapy. See your benefit booklet, section: Managed Care Authorization Program for more information.
CareFirst BlueCross BlueShield State of Maryland Member Service
Access our website at www.carefirst.com/statemd
File Breakdown
| Fact Name | Description |
|---|---|
| Form Identifier | The Maryland State Claim form is identified by the code CUT5803-1S and was last updated in October 2014. |
| Purpose of Form | This form is designed for members of the State Employees Health Plan to file claims for services rendered by non-participating providers of PPO, POS, and EPO claims. |
| Required Information | Key information required includes the subscriber and patient's legal names, membership number, relation to subscriber, and details of the medical service or supplies provided. |
| Submission Instructions | Claims must be submitted with itemized bills on the provider's letterhead, including descriptions of services, provider's diagnosis, date of service, and the charged amount for each service. Bills in foreign languages must be translated to English, and foreign currency converted to American dollars. |
| Additional Documentation for Certain Services | Claims for office visits, private duty nursing, durable medical equipment, X-rays, blood charges, and general anesthesia require specific additional information as outlined in the form. |
| Governing Laws and Warning | The form includes a warning that presenting false information is a crime potentially subject to fines and imprisonment. It authorizes the release of medical information necessary for the adjudication of the claim to CareFirst BlueCross BlueShield, an independent licensee of the Blue Cross and Blue Shield Association. |
Steps to Filling Out Maryland State Claim
After you receive medical treatment, especially from providers not participating within your health plan network, you must fill out a claim form to get reimbursed. This detailed guide provides straightforward steps to correctly complete the Maryland State Employees Health Claim Form. The process ensures your claim is processed timely and helps you avoid any errors that could delay payment. Remember to gather all necessary documents before starting, including itemized bills from your healthcare provider, and any additional documents required for specific types of services.
- Write down the Subscriber’s Legal Name including Last, First, and Middle Initial.
- Enter the Patient’s Legal Name as Last, First, and Middle Initial.
- Fill in the Membership Number.
- Select the Patient’s Sex by checking the appropriate box: Male or Female.
- Indicate the Patient’s Relationship to Subscriber by checking the correct box: Self, Spouse, Child, or Other.
- For the Subscriber’s Address, include Street, City, State, and Zip Code. Check the box if this is a new address.
- Enter the Patient’s Date of Birth, including Month, Date, and Year.
- Provide a Telephone Number where you can be reached.
- Write down the Group Number.
- Under the section titled "IMPORTANT," list any illnesses and the date of first symptom in the spaces provided. If more space is needed, attach a separate sheet.
- Answer yes or no to whether the treatment was a result of an injury, an automobile accident, work related, and whether the patient has Medicare.
- If applicable, indicate the Medicare Part A and Part B effective dates.
- Check if the patient is covered under another health insurance policy. If yes, complete the details regarding the policy holder, insuring company, policy or certificate number, effective date, type of coverage, and the coverage category.
- Provide the Name and Address of Policy Holder’s Employer if different from the subscriber.
- Sign and date the form at the bottom, certifying the information is accurate.
- Double-check if you have attached your itemized bills. This is crucial for the processing of your claim.
- Mail the completed form along with any required documentation to the address provided on the form: Administrator P.O. Box 14115 Lexington, KY 40512-4115.
Upon submitting your completed Maryland State Employees Health Claim Form with all the necessary documentation, your claim will be reviewed for eligibility and coverage under your plan. The review process includes verifying the provided information and ensuring all required details are present. Should further information or clarification be needed, you may be contacted. Once the review is complete, you will receive a notification regarding the decision on your claim, including any reimbursement amounts, if approved. It's important to keep a copy of all submitted documents for your records. Patience during this process is key, as thorough review is essential for accurate claim assessment.
More About Maryland State Claim
What is the purpose of the Maryland State Employees Health Claim Form?
This form is specifically designed for members of the State Employees Health Plan to submit claims when they receive medical services from providers who are not participating in the PPO, POS, or EPO networks. Such situations require members to directly file claims to seek reimbursement or payment for services rendered by out-of-network providers.
How do I accurately complete the Maryland State Employees Health Claim Form?
To properly complete the claim form, follow these guidelines:
- Ensure that all sections of the form are accurately filled out, including your legal name, membership number, and all relevant personal details.
- For each medical service or supply, include a detailed description, the date service was provided, the diagnosis, and the charge for each service.
- Attach original itemized bills and receipts for all services, ensuring they include the provider's full name, address, phone number, and if available, their CareFirst BlueCross BlueShield provider number.
- If you have coverage under another insurance plan, including Medicare, attach a copy of their payment statement or Explanation of Benefits (EOB).
What specific information must be included with claims for office visits, durable medical equipment, and other services?
When filing claims for specific types of services, additional information is required as follows:
- Office Visits: Indicate the type of visit (e.g., brief, intermediate, extended).
- Private Duty Nursing: Include dates and shifts worked, charge per shift, prescribing doctor's full name and degree, and the nurse's registration number.
- Durable Medical Equipment: Include the full purchase price for rented equipment, and a letter of medical necessity from your physician.
- X-rays: Specify the type of x-ray (e.g., chest, legs).
- Blood Charges: State the number of pints received, the charges for each, and the number of pints donated in replacement.
- General Anesthesia: Detail the length of time the patient was under anesthesia, in minutes.
- Accidental Injury Claims: Clearly indicate the date the accident occurred.
Is it required to sign the Maryland State Employees Health Claim Form?
Yes, the form must be signed by the subscriber. By signing, you certify that all the information provided is complete and correct. Furthermore, you authorize the release of any medical information necessary for the adjudication of the claim and acknowledge the legal implications of submitting false claims.
Should I attach my itemized bills to the claim form?
Absolutely. It is essential to attach your itemized bills to the claim form. These should be on the provider's letterhead stationary, detailing each service or supply provided, including the date, diagnosis, and the amount charged for each. Remember, bills in foreign languages must be translated into English, and charges in foreign currency converted to American dollars.
What should I do if I have coverage under another insurance plan?
If you have other health insurance coverage, including Medicare, indicate this on the form by checking "Yes" and providing the requested details about the policy. Also, as mentioned, include a copy of the Explanation of Benefits from the other carrier with your claim to ensure proper coordination of benefits.
Where do I send the completed Maryland State Employees Health Claim Form?
Once the form is completed and all necessary documentation is attached, mail it to the address provided for administrative use only, which is: Mail Administrator P.O. Box 14115 Lexington, KY 40512-4115. This ensures your claim will be processed by CareFirst BlueCross BlueShield, the service provider for the State Employees Health Plan.
Who do I contact if I have questions about completing the form or my claim?
For any questions regarding the form or your claim, you can contact CareFirst BlueCross BlueShield's State of Maryland Member Service at 1-800-225-0131. Additionally, you can find more information and resources on their website dedicated to State of Maryland employees at www.carefirst.com/statemd.
Common mistakes
Completing the Maryland State Claim form requires attention to detail. Common errors can lead to delays or denials of claims. Understanding these pitfalls is vital for a smooth processing experience.
Not updating personal information: A frequent oversight is failing to check the box if there's a new address. Your current contact details ensure timely communication and prevent mishandling of your claim.
Misidentifying the patient's relationship: Accurately stating the patient's relationship to the subscriber is crucial. Incorrect information here can lead to confusion and processing errors, especially when determining coverage eligibility.
Incomplete illness or injury details: Not thoroughly listing the illnesses or specifying the first symptom's date can obscure the claim's context. Similarly, incomplete details about accidents (when applicable) may hinder the assessment process.
Omitting other insurance information: If the patient has additional insurance coverage, failing to disclose this information can complicate the claim. Coordinating benefits between insurers is essential to determine the primary and secondary payers.
Forgetting to attach itemized bills or necessary documents: Submission without the required itemized bills or, when relevant, the Explanation of Benefits from another insurer, stalls the review process. Ensuring all documentation is attached verifies the services rendered.
Correcting these prevalent mistakes can significantly enhance the processing efficiency of your Maryland State Claim form. Careful review before submission helps avoid unnecessary delays, ensuring your claim is adjudicated promptly and accurately.
Documents used along the form
When preparing to submit a Maryland State Claim form for health benefits, it's important to gather all the necessary documentation to ensure a smooth and efficient processing experience. Alongside the claim form itself, several other documents and forms may often be required or prove helpful in supporting your claim. Understanding which documents to include can streamline the submission process and help avoid any delays.
- Itemized Bills: These are detailed bills from healthcare providers listing each service provided, the date of service, and the charge for each service. They should be on the provider's letterhead.
- Explanation of Benefits (EOB): If another insurance carrier, including Medicare, has already processed a claim, an EOB from that carrier should be included to detail what was covered and what remains the patient's responsibility.
- Letter of Medical Necessity: For certain claims, especially those involving durable medical equipment or special procedures, a letter from a healthcare provider explaining why the service or equipment is necessary for the patient's health can be crucial.
- Accident Reports: If the claim involves treatment for injuries sustained in an accident, a report or detailed account of the accident might be necessary. This is particularly relevant if the treatment is for injuries resulting from an automobile accident.
- Medical Records: Sometimes, especially for complex or ongoing medical issues, it may be necessary to include relevant medical records or a summary thereof that provides a context for the claim.
- Power of Attorney (POA) Documentation: If the claim is being submitted on behalf of the patient by someone other than the patient, documentation establishing the legal right to do so, such as a POA document, may be required.
Ensuring that you have the appropriate forms and documents in order can significantly impact the processing time and outcome of your Maryland State Claim form submission. Careful attention to the requirements detailed on the form and by your insurance provider can help facilitate a smoother claims process. Remember, it's always wise to keep copies of all documents submitted for your records.
Similar forms
The Maryland State Claim form is similar to other health insurance claim forms used throughout the United States, particularly those from other states and insurance providers. These forms often share a common structure, designed to collect necessary information to process health claims efficiently. Key elements include personal identification details for both the subscriber and the patient, information regarding the medical service or supply provided, including dates and charges, and detailed insurance policy information. This format ensures that all relevant data for adjudicating the claim is gathered succinctly, facilitating a smoother processing experience.
Specifically, the form mirrors the Uniform Health Insurance Claim Form used widely by private insurers and managed care organizations. Like the Maryland form, the uniform claim form includes sections for the provider's information, patient and subscriber details, and the charges for services rendered. What makes them similar is their purpose of enabling patients or healthcare providers to submit claims for medical services that are not directly billed by the healthcare provider to the insurance company. By requiring detailed healthcare service descriptions and the practitioner’s diagnosis, both forms aim to expedite the claim review process, ensuring accurate and timely reimbursement.
Another document resembling the Maryland State Claim form is the Workers' Compensation Claim Form that employees use to file for medical benefits following work-related injuries or illnesses. Despite different contexts—workers' compensation versus general health insurance—both forms collect detailed information about the nature of the injury or illness, the circumstances leading up to it, and the medical treatment received. This includes the identification of the patient and the healthcare provider, specifics of the treatment, and insurance details if applicable. The primary purpose here is to establish the validity of the claim and to ensure that it corresponds with policy coverage or workplace injury compensation guidelines, emphasizing the necessity for thorough documentation, whether the claim is related to general health or work-related incidents.
Dos and Don'ts
When filling out the Maryland State Claim form, it's important to ensure that the process is completed accurately and thoroughly to facilitate a smooth review and potential approval of your claim. To help guide you, here are several key do's and don'ts to consider:
- Do ensure that you correctly fill in the subscriber’s and patient's legal names, including the last name, first name, and middle initial, as inaccuracies here can lead to delays.
- Do complete every question on the form. Leaving out information can result in the rejection of your claim.
- Do indicate if the treatment was related to work, an automobile accident, or other specific circumstances as insurance coverage may differ based on these conditions.
- Do attach the itemized bills from your healthcare provider. These documents are crucial for the claim’s processing.
- Do sign and date the form. An unsigned form is not valid and will not be processed.
- Do not write in the spaces marked for administrative use only. These sections are intended for the insurance provider’s use.
- Do not forget to check whether any additional documentation is required for certain services such as durable medical equipment or accidental injury claims.
Remember, accurate and complete information supports the prompt processing of your claim. Keep copies of all documents submitted for your records.
Misconceptions
When navigating the complexities of submitting a health claim form for state employees in Maryland, there are a few misconceptions that often arise. It's important to address these misunderstandings to ensure that the process is as smooth and error-free as possible.
Only the subscriber needs to sign the form: A common misconception is that the Maryland State Claim form only requires the signature of the subscriber. In reality, the form mandates the signature of the person submitting the claim, which might be the subscriber, the patient, or a legal guardian, indicating that the information provided is accurate and complete.
You can submit without itemized bills if you provide a summary: Another misunderstanding is thinking a summary of services is sufficient for claim processing. The form explicitly requires itemized bills on the provider’s letterhead, including specific details like the date of service and the provider’s diagnosis, to properly process a claim.
It’s okay to submit the form without all information filled if you're unsure: Some believe it's acceptable to submit the form with incomplete information, planning to provide the missing details later. However, the form clearly states, “IMPORTANT: ALL QUESTIONS MUST BE ANSWERED”, underscoring the requirement to fill out every section to avoid delays in processing.
Translation of foreign bills isn’t necessary: There’s a misconception that foreign language bills don’t need to be translated. Contrary to this, the form requires that bills in a foreign language be translated into English, and foreign currency amounts converted to American dollars, ensuring the claims team can accurately assess and process the claim.
Electronic copies of bills are acceptable for submission: A common misunderstanding is the assumption that digital copies or scans of the original bills are acceptable. Yet, the instructions indicate that original bills and receipts are required for all services, emphasizing the need for physical documentation for a successful claim filing.
Understanding these key points can significantly improve the experience of dealing with health claims for Maryland State Employees, ensuring that your claims are processed efficiently and correctly.
Key takeaways
When members of the State Employees Health Plan in Maryland need to file claims for services received from non-participating providers, it is essential to understand the correct procedure for filling out and using the Maryland State Claim Form. The following key takeaways provide guidance on how to properly complete and submit this form:
- Properly identify the patient and subscriber: Ensure the subscriber’s and patient’s legal names are clearly printed, along with the patient’s relationship to the subscriber and other identifying information.
- Complete all required sections: All questions on the form, including those about the patient’s medical condition, whether the treatment was due to an injury or accident, and other insurance coverage details, must be answered.
- Disclose other insurance coverage: If the patient has additional health care benefits or services coverage, including Medicare, this information must be accurately provided in the designated section.
- Provide a detailed description of services: Attach bills that include the provider’s full name, the services or supplies provided, the dates of service, and the charges for each service. For services like office visits or private duty nursing, specific additional information is required.
- Convert foreign documents: Bills in a foreign language or currency must be translated into English and converted to American dollars.
- Attach itemized bills and receipts: Original bills and receipts for all services are required. Keep copies for your records. Each service or supply listed should have an accompanying description and charge.
Sign the form: The subscriber must certify the accuracy of the information provided by signing the form. This certification asserts that the claim is legitimate and that the benefits are only for charges incurred by the named patient. - Know the submission process: The completed form, along with all necessary documentation and itemized bills, should be mailed to the specified address. Remember to keep a copy of everything submitted for your records.
Correctly completing and submitting the Maryland State Claim Form is crucial for the timely processing of claims. For additional assistance or questions regarding the claim filing process, members can contact CareFirst BlueCross BlueShield Member Service or access more information through their website.
Common PDF Templates
University of Maryland Admission Requirements - Its comprehensive approach ensures that individuals are not only aware of their rights but are also guided through the admission process.
Printable New Employee Forms - Date of hire must be specified in the form, using the format mm/dd/yyyy.
Ccs Redetermination - Applicants must provide their academic intentions, including the degree or major they plan to pursue, to align financial support with educational goals.